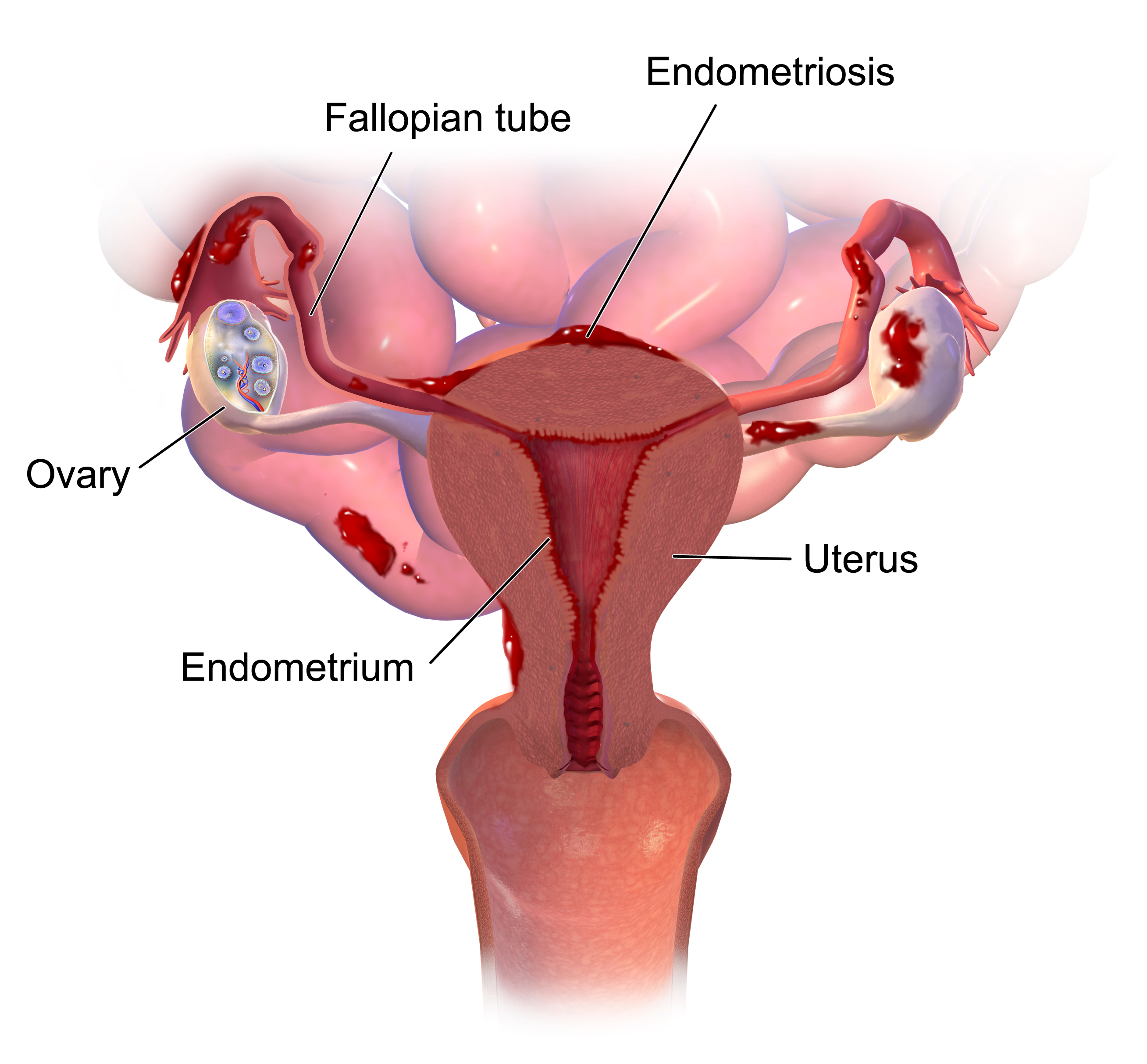
Endometriosis is a chronic condition in which endometrial tissue is located at sites other than the uterine cavity.
You’ve just been diagnosed with moderate endometriosis. You’ve been in excruciating pain for as long as you can remember, sometimes unable to keep food down because of it, and you’ve been bleeding for months without relief.
Now it’s time to choose a treatment plan. Do you get a hysterectomy? There’s no way you would be able to carry a child and the emotional and mental stress from surgery is intense. Do you get prescribed pain relief medication to deal with it? That doesn’t address the growing endometrial issue that can lead to cytotoxicity and reproductive cancers. Lastly, the main question in front of you: Do you start taking birth control to manage your hormone levels so you’re less likely to grow endometrial tissue? Can you even afford birth control where you are? Will you face judgement from those around you for taking it? Is it even worth it? These are the questions that are asked every day as women around America are diagnosed with abnormal uterine bleeding.
Abnormal uterine bleeding consists of disorders such as endometriosis, PCOS, heavy menstrual bleeding, and others, all entailing of symptoms such as irregular menstruation patterns, anemia, nausea, bowel dysfunction, or pelvic pain, many of which are so drastic that it prevents the patient from taking part in day to day activities. Much of this pain takes place in the uterus, as this is where the dysfunction occurs. While many of these disorders may have their variances of symptoms as whether there is endometrial tissue growing or ovarian cysts forming, the one commonality between them all: they all derive from an irregularity in sex specific hormones and have an effect on a female’s menstrual cycle. This is why birth control is an effective treatment for AUB.
Oral contraceptives work as they consist of both progesterone and estrogen hormones that lead to the thickening of the uterine lining and as you go into taking the fourth week of pills, you take a placebo that triggers “breakthrough bleeding” also known as menstruation, as the body is no longer being supplied the artificial hormones. In AUB, this is effective to maintain a more normal cycle and fluctuation of such hormones, preventing and treating some of the many symptoms of the disorders. If birth control is so effective in treating AUB disorders, why is there so much stigma and hesitation around it?
According to the New England Journal Medicine, the battle over the financial coverage has been a long one, but has significantly increased ever since the Affordable Care Act was passed in 2010. The Obama administration exempted houses of worship from the requirement of offering employee’s coverage of contraceptives. This is because while contraceptives help regulate menstruation, they also work to prevent pregnancies when sexually active, bringing in argument the churches disapproval of premarital sex.
The association between the “shame” of premarital sex and how it goes against religious values has led to many companies not financially covering contraceptives as medical treatment, stating that “If an employee wants birth control, that worker could … just work elsewhere”, thus a disparity in healthcare accessibility across America in these workplaces forms (Alta). These statements and views of the world may bring a perspective about the balance of religion in healthcare, but they also bring about healthcare disparities from their views on birth control.
In a study done in response to the Affordable Care Act, the inaccessibility of oral contraceptives (OCs) is greatly shown. The research done included those who took OCs for more than just to prevent conception, but for also AUB disorders and severe acne. After the coverage OC coverage exemption took place, this resulted in racial/ethnic minorities to be less likely to be OC users and to have a lower OCP usage if using, and minorities and married women were more likely choose more generic brands of OCs (Lin). This illustrates the decline in affordability of such treatments, as well as the increasing lack of accessibility to this treatment after the ACA was put in place, tying a direct relation between the decreasing contraceptive access and social stigma.
Should religiously affiliated institutions be exempt from providing coverage for contraceptives, even if they are used as a form of treatment? If we do not consider contraceptives to be part of the healthcare system, we then revert back to choosing unnecessary and irreversible invasive surgeries that devastate the human body, or to just leave patients that cannot afford those options to go suffer from AUB untreated. These options not only ignore the problem of AUB at hand, but also bring about unnecessary stress, pain, and declines the health of the patient as it progresses.
Without treating AUB directly we leave the patient not only to deal with the physical and mental burden that comes with the disorders, but they are also at risk to develop more destructive conditions such as cytotoxicity, where cell death or damage occurs in the body, take place. In a study by Dr. Donald P. Braun from The American Fertility Society, it was found that in patients with endometriosis, cytotoxicity towards normal cells was more likely to appear in patients that were untreated and later staged than in patients being treated by birth control. This ailment racks the human body; to have the ability to prevent this from occurring by using oral contraceptives is something that should not be overlooked and should never be withheld from a patient, no matter their economic status or religious affiliation.
These discussions of treatment are all contingent on people having an open line of communication with their physicians and being an advocate for their own health. As we delve more and more into the future of medicine, we must recognize the importance of making treatments accessible as well as being aware of the stigmas that surround our society that prevent us from receiving vital healthcare. One day you or a loved one could be sitting in a room fighting to overcome the healthcare obstacles in your way to get the best treatment, but if we keep an understanding and educated mind about ourselves, then we can help prevent so much pain and provide patients with actual choices.
By: K. Peck
References
- Alta, C. R. (2012). Warning: Contraceptive drugs may cause political headaches. The New England Journal of Medicine, 366(15), 1361-1364. doi.org/10.1056/NEJMp1202701.
- Bradley, L. D., & Gueye, N.-A. (2016). The medical management of abnormal uterine bleeding in reproductive-aged women. American Journal of Obstetrics and Gynecology, 214(1), 31–44. doi.org/10.1016/j.ajog.2015.07.044.
- Braun, D. P., Gebel, H., Rotman, C., Rana, N., & Dmowski, W. P. (1992). The development of cytotoxicity in peritoneal macrophages from women with endometriosis. Fertility and Sterility, 57(6), 1203-1210.
- Lin, H.-C., & Lee, H.-Y. (2015). Utilization of and Adherence to Oral Contraceptive Pills and Associated Disparities in the United States: A Baseline Assessment for the Impact of the Affordable Care Act of 2010. International Journal of Health Services, 45(4), 729–742. doi.org/10.1177/0020731415591244.
Image Credits
- Blausen, Picture of uterus with endometrium, TeachMeObGyn, https://teachmeobgyn.com/gynaecology/uterine/endometriosis/.